
What is a Cataract?
Cataract is a condition of clouding of the natural lens that resides within the eye. Its normal function is to focus the incident light beams entering the eye through the cornea onto the fovea of the retina, where specialised photoreceptors reside and, through geometric isomerisation of the retinal chromophore, send information about the incident light intensity and frequency to the brain for further processing. When the lens clouds, the incoming light is both decreased in intensity and distorted leading to the distorted perception of the external world by the patient.
Prior to 1700, it was thought that the cause of cataract was opaque material flowing through the central lens itself, as it was observed that there was a central visual defect and patients would have a whitening of the lens itself (1). Through modern scientific method, we have been able to discover that cataract is a diverse group of disorders with their own associations that lead to a clouding of the lens. The most common cause is degeneration of the proteins found in the centre of the lens leading to hardening and discolouration (yellowing), which can paradoxically increase the refractive power of the lens and patients who previously relied on reading glasses no longer need to in later stages of the disease. Risk factors associated with cataract development include ultraviolet – B exposure, cardiovascular disease, diabetes, glucocorticoid use, ionising radiation exposure and ocular inflammation.
Cataract Surgery through the ages
As the ophthalmic historian Julius Hirschberg wrote, “At the present time, it is impossible to answer this important historical question as to which nation (or even which man) first performed a cataract operation.” Evidence of early use of surgical technique to treat cataract and restore sight can be found across a variety of civilisations in the ancient world. The similarities in technique used across these cultures in both the East and West point to the probability that it was developed at one place and spread, as opposed to independently being created in multiple times and places (2).
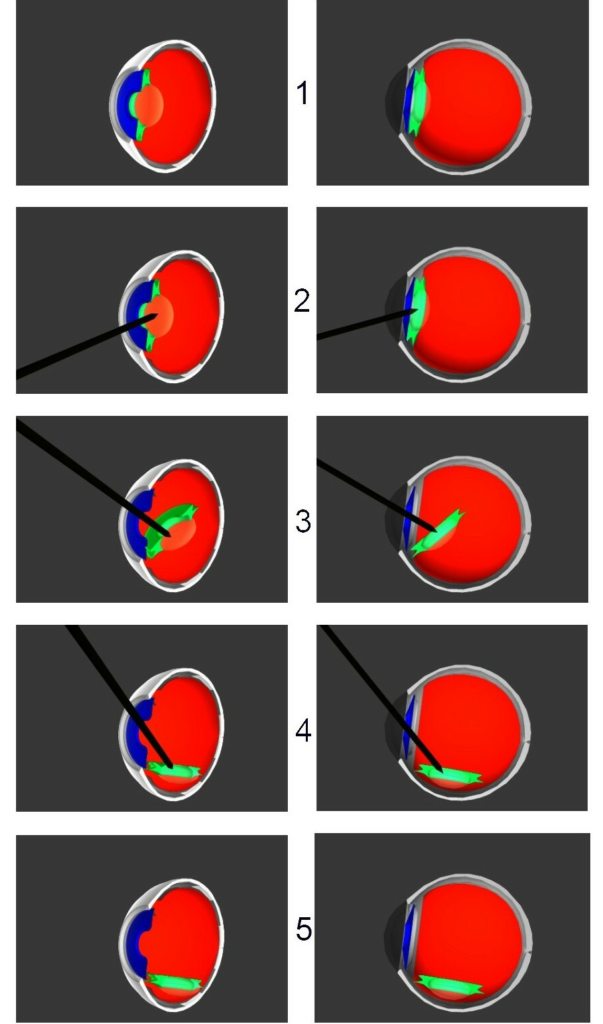
The earliest and most widespread technique used in the ancient world was coaching (see Figure 1). This involved using a sharp instrument, usually made of bronze or silver, to make an incision at the limbus and dislodge the cataract by destruction of the zonular fibres. The resultant lens would then reside within the vitreous humour and there would be an unobstructed path for light to now reach the retina (3).
The earliest theorised use of coaching is thought to be from the Ancient Egyptian civilisation. The first documented case of cataract is on a statue from the 5th dynasty (around 2457 BC) and is a wooden statue of a priest reader with a clear white patch carved into the pupil of the left eye, thought to represent a cataract. Treatment of this disease is also represented in this era, with copper probes found in the tomb of King Khasekhemwy, and in the tomb of Skar in Cairo, one of the chief surgeons was found to be buried with several bronze instruments. However, rods and probes can be used for other medical and non-medical applications such as application of ointments, removal of foreign bodies and scraping the eye, the significance of these discoveries in the history of cataract surgery is still unknown. Another famous reference to the existence and treatment of cataract in the ancient civilisations is also found in the Babylonian Code of Hammurabi (4)., This is a collection of 282 laws of established standards for commercial interaction with defined punishments. One of such laws dictates that a doctor who caused their patient to lose an eye from surgery should be destined to have their hands cut-off. The underdeveloped nature of this technique would lead to poor visual outcomes. Complications such as secondary glaucoma, endophthalmitis and hyphema would often lead to blindness of the patient, despite the reasoning for the intervention was to cure blindness (5).
Detailed documented evidence of cataract extraction technique was first done by the Indian surgeon Sushrata in the ancient Sanskrit text Sushrata Samhita. Amongst a variety of topics that we still use in modern surgical practice including rhinoplasty and skin flap creation, Sushrata outlined a modified Extracapsular Cataract Extraction (ECCE) technique where a needle is inserted and used to pierce the anterior capsule and the same instrument is used to disrupt the lens. Next, the patient is instructed to perform a Valsalva Manoeuvre to anteriorly dislodge the dense lens fragments into the anterior chamber. In the post-operative period, the patient’s eye would be dressed in leaves and encouraged to lie flat and not partake in strenuous exercise like coughing or sneezing (6).
As knowledge on ocular anatomy and cataract physiology improved, so did the surgical techniques used to treat the disease. Almost 23 centuries after Sashruta outlined his technique, a French surgeon named Jacques Daviel documented his new procedure, more akin to the modern method of ECCE. He would make a corneal incision > 10 mm at the 6 o’clock mark of the limbus with a corneal knife, then use a blunted needle to puncture the anterior lens capsule. A spatula and a curette were used to extract the lens. Akin to Sushrata’s post-operative care, patients were dressed in a bandage soaked in wine and lay in a dark room for a few days. Despite this being a great advancement for cataract technique, concerns remained from this procedure notably uveitis from retained cortex and a high incidence of posterior capsular tears due to the instrumentation of the lens itself (7).
Not long after, in 1753, a London surgeon names Samuel Sharp documented a new technique of Intracapsular Cataract Extraction (ICCE). With this technique, the whole lens and its capsule were removed a large limbal incision. The original method used by Samuel Sharp involed the use of forceps to fracture the zonular fibres holding the capsule in place, but this evolved to the use of the enzyme alpha-chymotrypsin by Joaquin Barraquer in 1957. Further refinement of ICCE technique was with the use of cryoextraction; the use of a frozen probe to gently evacuate the cataract from the eye. Advancements in modern anaesthetics and sterilisation served to make this technique more popular, however its popularity declined as ECCE technique was refined. The main drawbacks of ICCE ae due to the removal of the lens-capsule complex, which physiologically serve as a barrier of posterior and anterior structures of the eye. Removal of this results in potentially blinding complications such as retinal detachment, vitreous prolapse and corneal decompensation. The other main drawback is that the large corneal incision required leads to a greater degree of astigmatism once healed (8).
Up until this point, patients treated with surgery for cataract were left without a refractory lens (aphakic), meaning that for any meaningful vision to be achieved in the treated eye, a high-powered hyperopic lens needed to be used to focus images on the retina. Sir Harold Ridley noted that WWII pilots were able to tolerate small shards of the plastic Polymethyl Methacrylate (PMMA) from air fighter shattered cockpits within their anterior chamber. This led him to develop the first Intraocular Lens (IOL) and first implanted this in 1949. Initial backlash of the technique was justified due to the considerable post-operative complications including uveitis, glaucoma and dislocation of the lens. However, as technique for cataract extraction developed, so did the required IOL used, including individualised lenses according to required power, creation of lenses to sit behind the iris and in the capsular bag itself (9).
In 1967, the American ophthalmologist Charles Kelman introduced phacoemulsification (“phaco”) as an alternative to ECCE to allow for drastically smaller corneal incision. This technique uses an ultrasound-powered probe to simultaneously break up the cataract within the capsule with minimal disturbance of the zonular fibres, and aspiration of the cataract remnants. This decreases the limbal incision from 10mm required to fit the entire lens through, to 3-4 mm (10).
Another key development came with the introduction of ophthalmic viscoelastic devices (OVDs) in 1972. This is a gel-like substance used simultaneously with the phaco device to ensure that the stability of the anterior chamber is maintained throughout the procedure. This would allow an easier surgical field for the ophthalmologist to work in but also protect internal structures, thus minimising complications (11).
Conclusion
Cataract surgery can be considered as one of the most successful medical interventions designed to improve the quality of life of the patient. Current cataract techniques involved meticulous breaking down and extraction of the lens with implantation of a customised IOL for the patient’s refractory needs, which can all be achieved with minimal time in the operating theatre. However, despite these advances, primitive techniques such as couching are still practiced in rural populations where availability of medical resources and infrastructure is limited. Further work needs to be done to extend ophthalmic services to these communities, with the right health education, to let all of humanity benefit from the generational innovations in cataract management.
References
- Ruparelia, S. (2022). A lens into the past: The history of cataract surgery. DALHOUSIE MEDICAL JOURNAL, 48(1).
- Leffler CT, Klebanov A, Samara WA, Grzybowski A. The history of cataract surgery: from couching to phacoemulsification. Ann Transl Med. 2020 Nov;8(22):1551.
- Ruparelia, Sunil. (2021). A lens into the past: The history of cataract surgery. Dalhousie Medical Journal. 48. 4. 10.15273/dmj.Vol48No1.11257.
- Blomstedt P. Cataract surgery in ancient Egypt. J Cataract Refract Surg. 2014 Mar;40(3):485-9. doi: 10.1016/j.jcrs.2014.01.006. Epub 2014 Jan 31.
- Ascaso FJ, Lizana J, Cristóbal JA. Cataract surgery in ancient Egypt. J Cataract Refract Surg. 2009 Mar;35(3):607-8.
- Raju VK, Raju LV. Cataract surgery and controversy: Susruta-Daviel-Kelman. Indian J Ophthalmol. 2017 Dec;65(12):1275-1276.
- Davis G. The Evolution of Cataract Surgery. Mo Med. 2016 Jan-Feb;113(1):58-62.
- Hubbell AA. Samuel Sharp, the first surgeon to make the corneal incision in cataract extraction with a single knife: A biographical and historical sketch. Med Library Hist J. 1904;2(4):242, 1–268.
- Apple DJ, Sims J. Harold Ridley and the invention of the intraocular lens. Surv Ophthalmol. 1996;40(4):279–292.
- Kelman CD. Phaco-emulsification and aspiration: a new technique of cataract removal: a preliminary report. Am J Ophthalmol. 1967;64(1):23–35.
- Davis G. The Evolution of Cataract Surgery. Mo Med. 2016 Jan-Feb;113(1):58-62.